")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Comprehensive Custom-Pak® in Cataract and Vitreoretinal Surgery in Canadian Hospitals: Time and Budget Impact Analysis
Authors Punch D, Davis JS , Hahn R , Gill R, Hsiao CW, Kara R
Received 16 November 2022
Accepted for publication 8 February 2023
Published 1 March 2023 Volume 2023:15 Pages 151—164
DOI https://doi.org/10.2147/CEOR.S397671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Donna Punch,1 Jonathan S Davis,2 Rebecca Hahn,2 Rav Gill,3 Chia-Wen Hsiao,4 Richard Kara4
1Kensington Eye Institute (Retired), Toronto, Ontario, Canada; 2KJT Group, Inc, Rochester, NY, USA; 3Alcon Canada, Inc, Mississauga, Ontario, Canada; 4Alcon Vision LLC, Fort Worth, TX, USA
Correspondence: Donna Punch, Tel +1 905-238-3228 ; +1 647-980-7716, Email [email protected]
Purpose: Surgical procedure packs are commonly used in ophthalmological surgeries, but quantitative evidence demonstrating the time efficiency and economic impact of their use is limited. Evaluating the time and cost of surgical pack use is particularly important for publicly funded healthcare systems with tight budgets and/or an emphasis on value-based care. This study sought to estimate the economic impact of comprehensive surgical pack use in cataract and vitreoretinal (retina) surgeries across operating room (OR), materials management, and accounting departments in Canada.
Methods: A budget impact model developed for the United States (US) from a self-reported cross-sectional study was adapted for Canada. The US study obtained data via an online survey and timing exercises of surgical procedures. The model was adapted using relevant Canadian-specific labor and cost inputs. Use of generic commodity packs (no proprietary equipment-specific supplies) was compared to full utilization of Custom-Pak®, a comprehensive pack (disposables plus equipment-specific supplies) in cataract and retina surgeries at the facility and aggregate group (provincewide) levels.
Results: Switching from generic to comprehensive pack use in all 2500 cataract procedures at a community hospital saves 287 labor hours per year, primarily in the materials management department. Surgery preparation (OR) hours saved allow for an additional 196 potential procedures annually. Most of the Canadian Dollar (CAD) $39,815 annual cost savings are realized for the OR. Aggregating across 50,000 cataract surgeries at the provincial level yields savings of 5608 hours and 3916 additional procedures, translating to hidden cost reductions of CAD$790,632 annually. Implementing full Custom-Pak use at the facility level in 1000 retina cases saves $10,650 annually; provincewide, 127 potential additional procedures can be gained.
Conclusion: Comprehensive Custom-Pak use improves efficiency in cataract and retina surgeries saving substantial time and cost in Canadian hospitals, potentially allowing more patients to have these procedures, and reducing wait times.
Keywords: cataract, retina, surgical instruments, economic models, Canada, hospital materials management
Introduction
The implicit costs of managing materials and preparing for cataract/anterior segment and retinal/posterior segment surgical procedures are often unquantified at a given facility or at the health system level.1 Understanding these costs is important for hospital and health system administrators to make informed decisions regarding the procurement and use of surgical products and services. Surgical procedure packs (“surgical packs”) are expected to improve surgical efficiency by streamlining materials management and surgery preparation. The composition of surgical packs can vary; those used in cataract and vitreoretinal (retina) surgery can include only “pure disposable” (or consumable) supplies, while comprehensive packs include both pure disposable supplies and sterile equipment-specific surgical disposable supplies.2 Surgical packs can be off-the-shelf that include a specified set of disposable supplies or can be customized for a surgeon or surgical team.
Despite extensive use of surgical packs in healthcare facilities, the literature is limited in demonstrating their economic impact. Previous studies have found that decreasing non-operative time can reduce operating room (OR) staffing costs3 or increase the number of surgical cases.4 Custom surgical packs can reduce the handling of surgical supply material for surgical preparation in the OR and streamline storing and pulling supplies.5 A study of custom surgical splint packs for orthopedic surgeries found a significant reduction in time spent on retrieval of supplies and preparation compared to conventional gathering and preparing of bulk supplies.6 Research on the impact of surgical packs in ophthalmological procedures is from 2004 or earlier and limited in scope. The hidden costs of ordering a single item (angled blade) used in cataract surgery were calculated in 1995 to demonstrate the per procedure costs associated with the ordering, billing, handling, storage, and preparation of the item across hospital departments.1 An exploratory time and motion study presented in 2004 demonstrated time and cost savings with use of Alcon’s Custom-Pak® surgical pack (Alcon Vision LLC, Fort Worth, Texas, US) in cataract surgery in two hospitals in France.7 To our knowledge, use of custom packs and their potential benefits have not been explored in Canadian healthcare facilities for cataract or retina surgeries.
Canada has a decentralized and publicly funded healthcare system. Provincial and territorial governments are mandated to provide medically necessary services to all their citizens free of user charges.8 Canadian hospitals are independent non-profit corporations that account for 26.4% of public health expenditures in Canada.9 Cataract surgery has been financed through a bundled payment mechanism called Quality Based Procedures (QBP) in the largest province of Ontario since it implemented Health System Funding Reform in 2012.10 Under QBP, Ontario hospitals are allocated a quota for cataract surgeries and provided a fixed payment for each surgery performed. Supplies, such as those used in performing cataract and vitreoretinal surgery, are typically sourced using request for proposals, or tendering.12
In a healthcare environment with emphasis on value-based care, it is important to understand hidden costs and assess opportunities for increasing efficiencies. This is particularly critical as the prevalence of the major causes of vision loss including cataracts, age related macular degeneration, and diabetic retinopathy, are expected to increase by more than 40% between 2019 and 2050,13 driving demand for treatments, including surgical procedures.
The goal of our research is to understand the impact of comprehensive Custom-Pak on the implicit costs of cataract and retina surgery in Canada, adapting a model developed for the United States (US). Using a robust data collection approach from a US cross-sectional study coupled with Canadian government and facility-level hospital data, we present an economic evaluation of the impact of surgical pack use in a Canadian healthcare setting to better inform hospital and group purchasing organization procurement decisions and potentially improve the quality of ophthalmology care.
Materials and Methods
Overview
To estimate the time and cost impact of surgical pack use in cataract and retina surgery across OR, materials management, and accounting departments, we adapted a budget impact model (BIM) previously used to assess the economic impact in the US16 to the Canadian setting. The model was based on a self-reported cross-sectional study conducted in the US between June 28, 2019, and August 12, 2019. Inputs were gathered for the development of the BIM via an online survey among surgical technicians and supply chain managers representing 99 US facilities across hospital and ambulatory care settings. The US study was reviewed by the Western Institutional Review Board and determined to be exempt because the survey was anonymous with adequate protections in place to protect participant privacy and maintain data confidentiality. The study was conducted in accordance with the Declaration of Helsinki. Time assessments for the entire within-facility lifecycle were quantified, from supply price negotiation and ordering through receiving, stocking, pulling, and preparing the surgical field to the start of the procedure. Additionally, a timing exercise was completed by surgical technicians for several procedures at their facility during the same time period (June 28, 2019, and August 12, 2019) and were used to calculate the duration of surgical preparation and the procedure itself; surgical supply use from comprehensive Custom-Pak and other sources was also recorded. Custom-Pak was evaluated as it is the most comprehensive ophthalmological surgical pack available; equipment-specific and disposable supplies are optimally arranged and individually customized for the surgical team and for the procedure.
A BIM was developed to estimate time spent and labor costs of surgery preparation and materials management for a representative US facility, defined by the mean data reported in the US analysis, across three departments. The model uses the mean time spent for each task across the supply’s life cycle for each supply type to calculate the total time spent both with and without comprehensive Custom-Pak use. Time expenditures were calculated at the per procedure level and tallied to assess the annual time estimates; these were assessed for each department and for the facility overall. Hidden costs, defined as those incurred due to labor, storage, and freight use, were calculated. The BIM developed for the US study was adapted to include relevant procedural, facility, and labor inputs to reflect the Canadian healthcare landscape, from the perspective of hospital administrators and provincial governments. The BIM for Canada was adapted for hospital facilities only. An overview of the processes reflected in the model structure is presented in Figure 1; the model structure is displayed in Figure 2.
 |
Figure 1 Cataract and vitreoretinal surgery processes reflected in the budget impact model. Overview of the processes reflected in the budget impact model structure across accounting, materials management, and operating room departments. |
 |
Figure 2 Cataract and Vitreoretinal Surgery Budget Impact Model Structure. The budget impact model takes time spent and costs measured at the individual surgical supply level for tasks completed over the supply life cycle and aggregates them into their respective departments and ultimately to the facility level. Information in parentheses reflects the data source for cost, time per task, and number of people assigned to each task. *Tasks include time and cost for each disposable surgical item. Abbreviations: KEI, Kensington Eye Institute; US, United States. |
Model Parameters
Inputs for the original model were obtained from the US survey and timing exercises and included time spent in OR, materials management, and accounting tasks across 21 and 17 categories of surgical supplies that are typically used in cataract and retina surgery practices, respectively (Table 1). In the hospital setting, 46 US respondents completed the survey for cataract procedures and 41 provided information for retina procedures; technicians timed 140 cataract and 140 retina surgeries. Parameters adapted for Canada include percentage of procedures using comprehensive Custom-Pak, cost of taxes and benefits as a percentage of salaries, OR preparation time between cases, time to verify and pay invoices, and the number of people involved in certain tasks across departments; these inputs were based on historical data from the Independent Health Facility, Kensington Eye Institute (KEI, Toronto, Ontario)17 (Table 1). Historical data (D. Punch, personal communication, April 2021) reporting the cost per case from KEI was used to calculate the overhead cost per hour for the OR, which was then updated to reflect 2018 labor costs. Storage space costs were based on the rental rate for access to the facility and were also ascertained from KEI (D. Punch, personal communication, April 2021). Other facility parameters such as reimbursement rates, average yearly hours worked, and salaries of staff involved in ophthalmological procedures were obtained from the Ontario Ministry of Health and the government of Canada (Table 1). Publicly available data used in the model is presented in Table S1).
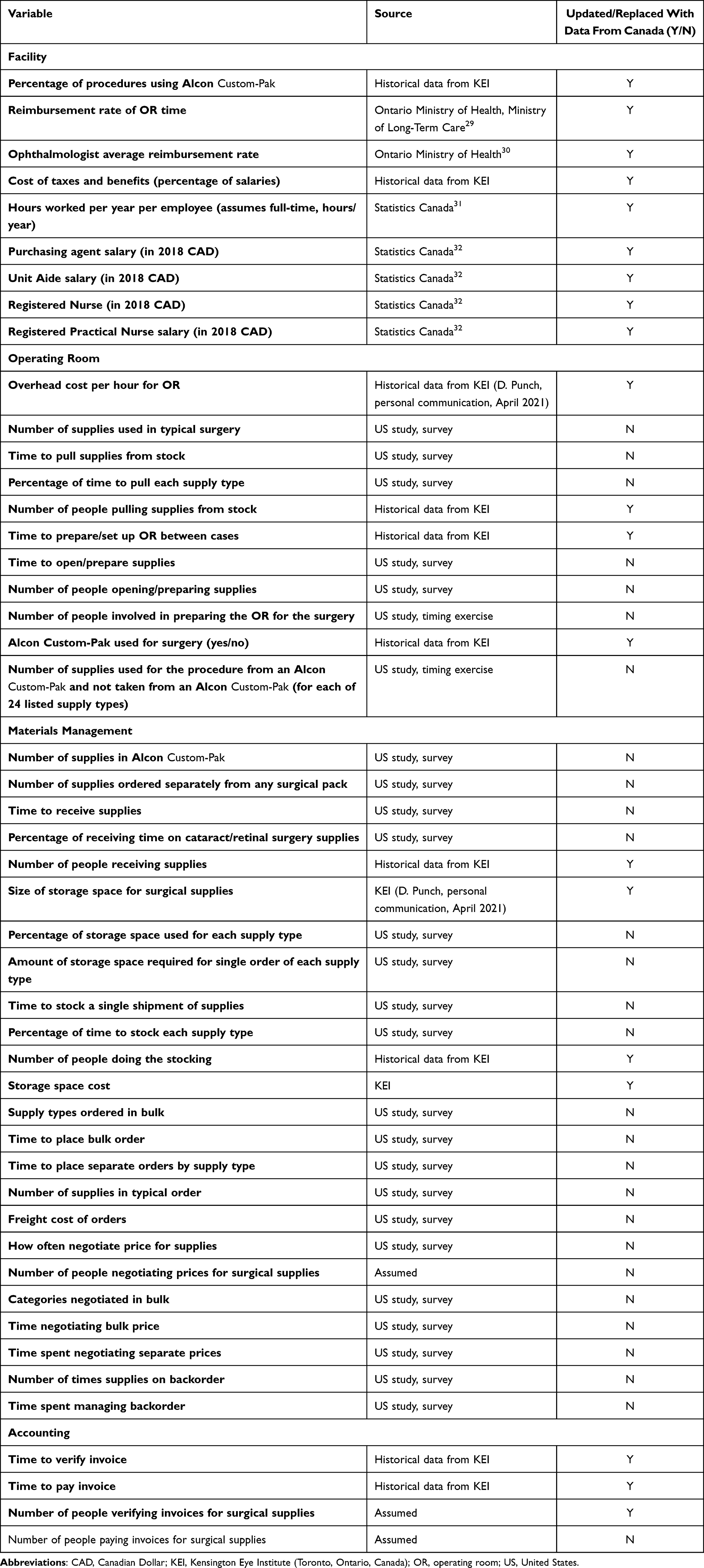 |
Table 1 Cataract and Retina Surgery Budget Impact Model Inputs |
Time and Cost Estimates
The number of surgical supply orders was calculated as follows:

Time estimates were calculated both for surgeries using comprehensive Custom-Pak and those not using Custom-Pak. To estimate the cost for surgeries with and without comprehensive Custom-Pak, the total cost for each task, total costs for storage, and total cost of freight were calculated as follows:



Surgeries using comprehensive Custom-Pak and those not using Custom-Pak were combined to get annual totals for each task by department (OR, materials management, accounting) and facility level. Per procedure time and cost estimates are averages across all surgeries at the facility.
Time and Cost Scenarios
To quantify the benefits of using a comprehensive customized surgical pack, we examined the impact of transitioning from use of “generic commodity packs” (no equipment-specific supplies) in all procedures to 100% use of a “comprehensive pack” that includes pure disposables and additional equipment-specific supplies (comprehensive Custom-Pak) in two cataract and two retina scenarios: 1) cataract procedures at the facility level (community hospital) with 2500 cases/year; 2) cataract procedure at the aggregate level (provincewide) with 50,000 cases/year; 3) retina procedures at the facility level (community hospital) with 1000 cases/year; and 4) retina procedure at the aggregate level (provincewide) with 10,000 cases/year. The number of cases in our scenarios are examples to illustrate caseloads in a “typical” province in Canada, since caseloads vary across the country. Time and cost impacts are the difference between the estimates for each of the four scenarios, which follow the same general formula: 
We defined total surgery preparation time savings as the difference between the total time per year spent on surgery preparation in the comprehensive pack use scenario and the corresponding time spent in the generic commodity pack use scenario. Per procedure surgery preparation time is defined as the average surgery preparation time multiplied by the proportion of surgery preparation time used for opening or preparing surgical supplies and for all other surgery-related preparation tasks. “Potential Additional Procedures” is the amount of time saved in surgery preparation divided by the typical amount of time to prepare and complete a procedure (which is composed of time to prepare for the procedure plus the time to perform the procedure, including the time needed for operating room sanitation in between procedures). To account for outliers and the potential for self-report bias to overestimate time and cost estimates, we winsorized the data above the 80th percentile for the data collected in the US survey and timing exercise.
Sensitivity Analyses
We conducted three sensitivity analyses to further test the BIM and its credibility by determining the possible boundaries of the model. These analyses evaluate the range of possible outcomes when varying only 1) the job title (and associated salary) of the staff assigned to complete the task, 2) the number of personnel assigned to complete the task, and 3) the percent change in all costs (storage, freight, OR overhead, and labor), recording the impact of using comprehensive Custom-Pak relative to the generic commodity pack while keeping all other variables constant in each analysis. For the task assignment analysis, we iterated each task measured in the model across all job titles for each task. The personnel sensitivity analysis starts from a single staff member assigned to each task and then adds additional staff to the task until there are twice as many people doing the task as are assigned in the scenario’s initial configuration (eg, if the hospital originally had two people pulling supplies, the analysis would use one, two, three, and four people sequentially for that task). Lastly, we assessed the impact of varying all costs (Canadian Dollar; CAD) of the procedure from −50% to +50% relative to generic commodity pack usage, in increments of 1% throughout the range.
Results
Cataract Procedures
Switching from generic commodity pack use to comprehensive Custom-Pak use in 2500 cataract surgery cases in the community hospital setting saves 6.90 minutes per procedure, primarily for the materials management department (Table 2). Time savings in preparing for surgery are also substantial, at 1.86 minutes per procedure and 77.5 hours annually (Table 2), translating to 196 potential additional procedures and almost CAD$40,000 in hidden cost reductions at the facility level (Table 2). At the aggregate level with 50,000 cases per year, 1550.0 hours of surgery (OR) preparation are potentially saved annually (Table 3), translating to 3916 potential additional procedures. Over CAD$790,000 in hidden costs can be decreased annually with full comprehensive pack use, provincewide (Table 3). Assuming one comprehensive Custom-Pak is used in a procedure, the potential time savings associated with 13 Custom-Paks saves time equivalent to one additional cataract surgery (including time to turn over the OR and perform the surgery).
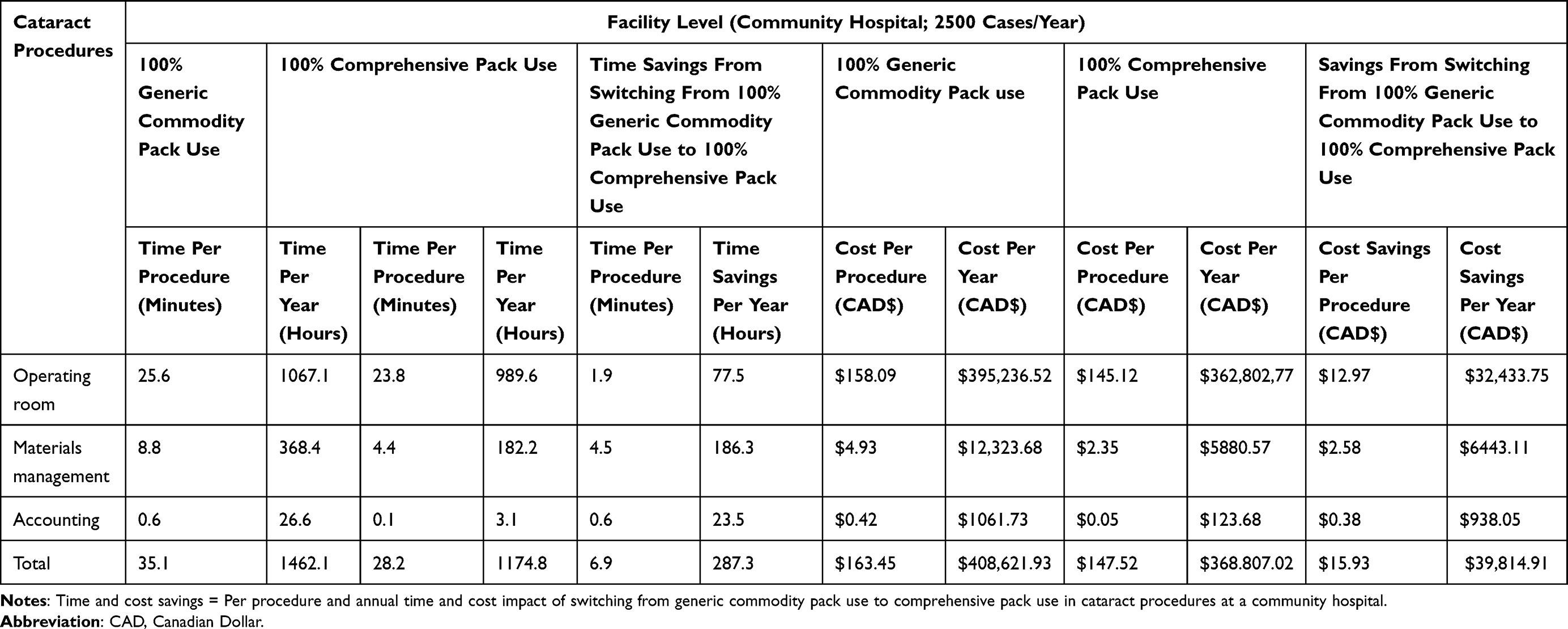 |
Table 2 Time and Cost Impact of Comprehensive Pack Use in Cataract Procedures at the Facility Level |
 |
Table 3 Time and Cost Impact of Comprehensive Pack Use in Cataract Procedures at the Aggregate Level |
Retina Procedures
Switching from generic commodity pack use to comprehensive Custom-Pak use in 1000 retina surgery cases in the community hospital setting saves over 2 minutes per procedure, or 41 hours annually (Table 4).
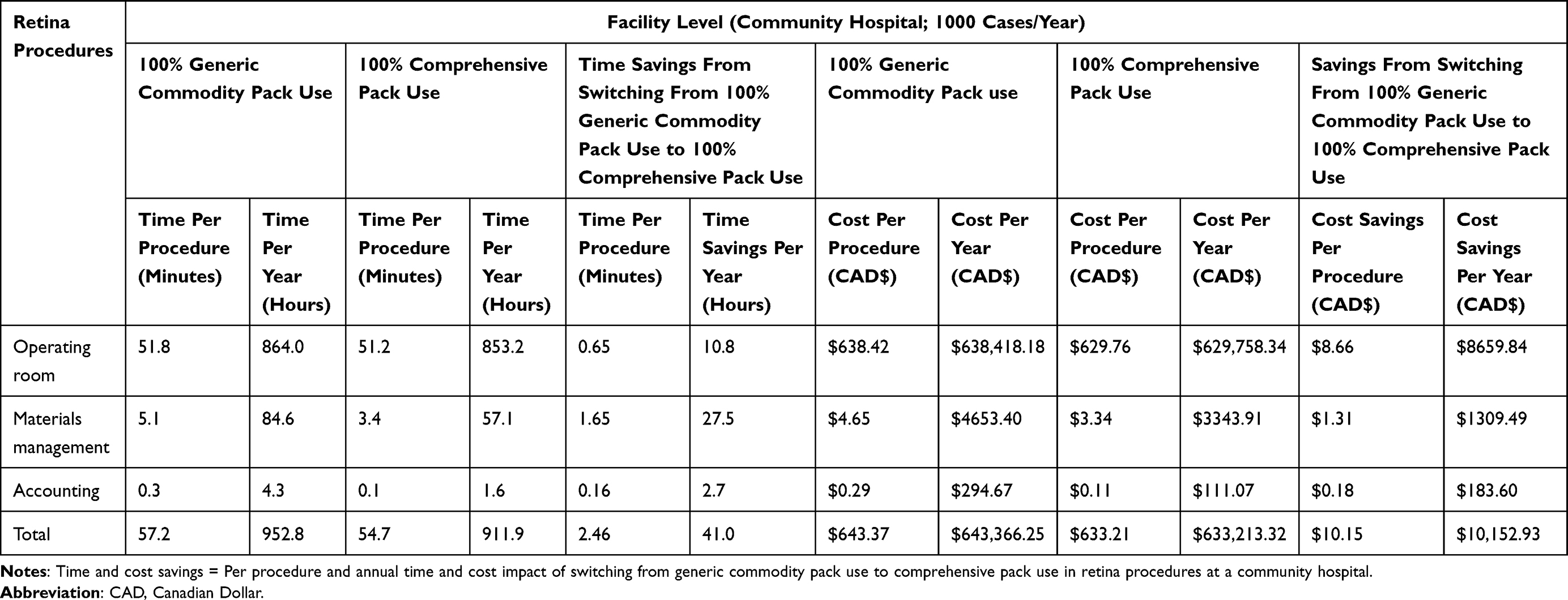 |
Table 4 Time and Cost Impact of Comprehensive Pack Use in Retina Procedures at the Facility Level |
At the aggregate level with 10,000 cases per year, 108.3 hours of surgery preparation are saved annually (Table 5), translating to 127 potential additional procedures. Annual hidden cost reductions of transitioning to full comprehensive pack use are approximately CAD$106,000 provincewide (Table 5). With one comprehensive Custom-Pak per procedure, the potential time savings associated with 79 Custom-Paks saves time equivalent to one additional retina surgery (again including turning over the OR and performing the surgery).
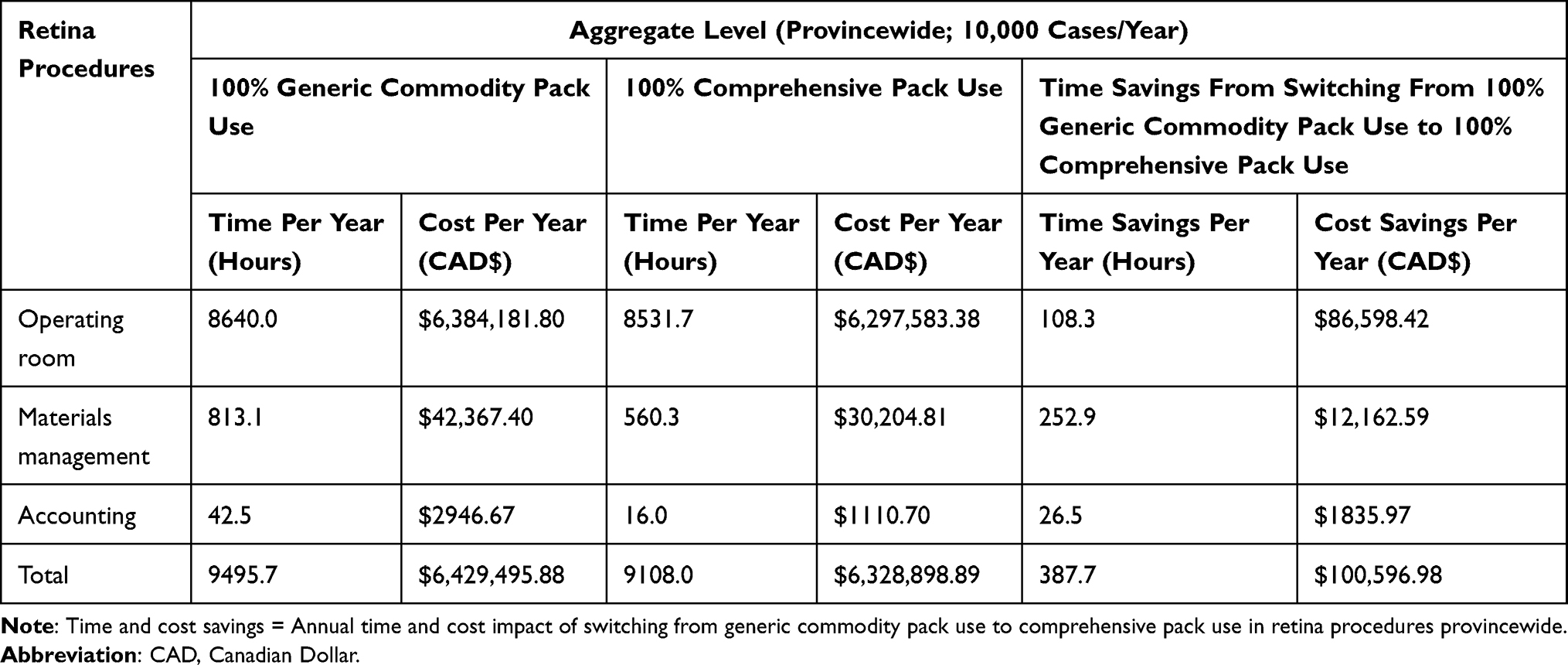 |
Table 5 Time and Cost Impact of Comprehensive Pack Use in Retina Procedures at the Aggregate Level |
Sensitivity Analyses
The task assignment sensitivity results representing the annual cost savings by department are displayed in Figures S1 and S2 for cataract and retina procedures, respectively. Although staff roles with higher salaries, such as a registered nurse, show increased savings because they are more costly to employ for certain tasks, the overall cost savings do not vary substantially when switching task assignments between hospital staff. Figures S3 and S4 illustrate the personnel sensitivity results, demonstrating that the impact of using comprehensive Custom-Pak versus a generic commodity pack are substantial and are generally not sensitive to the number of people working on a particular task outside of pulling surgical supplies and placing orders for supplies. Reducing the total costs for conducting cataract and retina procedures in a community hospital in Canada by 50% (CAD/hour) still results in considerable cost savings annually – $20,269.62 and $5660.06, respectively (Figures S5 and S6).
Discussion
Increasing efficiency in the provision of healthcare is particularly important in a publicly funded value-based healthcare system. Surgical pack use improves the efficiency of surgical preparation by eliminating the need to individually unwrap, sort, and organize each supply used in a procedure.5 We hypothesized that transitioning from generic commodity pack use to comprehensive pack use at the community hospital level would provide time efficiencies resulting in hidden cost savings that would be magnified at the aggregate provincewide level.
In this study, we adapted a model designed to assess the economic impact of comprehensive Custom-Pak in the US to the Canadian setting. Fully utilizing comprehensive Custom-Pak in community hospitals results in substantial annual time and hidden cost savings, which is consistent with other research examining the impact of surgical packs in a limited number of sites in ophthalmological procedures,1,7 orthopedic surgeries,6 and cardiac surgery.18,19 Although the bulk of labor hours saved are in the materials management department, time savings gained from more efficient surgery (OR) preparation with full comprehensive Custom-Pak use would potentially allow nearly 4000 more patients to receive cataract surgery each year and 127 more patients to have retina procedures provincewide; this demonstrates that additional government funding is warranted to enable hospitals to conduct more procedures and adopt new technologies. During the tendering process, a facility can request additional funding from the government if it can prove additional capacity. Our model demonstrates potential additional capacity; a surgeon can conduct more surgeries if barriers, such as the surgical supply preparation time, are reduced.
Hidden cost savings are nearly CAD$40,000 annually at the hospital level for cataract surgery, primarily for the OR department, which can be extensive. Transitioning to Custom-Pak can allow facilities to conduct more cataract surgeries without substantial capital investments20 (D. Punch, personal communication, April 2021). Due to the specialized nature of retina procedures, the number of facilities conducting these surgeries is limited. However, the amount of disposable surgical instruments associated with retina surgeries is greater than those associated with cataract surgeries and thus, streamlining the surgical supply preparation process can be particularly beneficial. Although direct costs such as that of the surgical supplies was not assessed in our model, if the direct cost differential between Custom-Pak and a generic commodity pack is less than the time savings/cost calculation, Custom-Pak would be more efficient. If, however, the direct cost differential between the two packs is more than the time savings/cost calculation, two possibilities remain: either the configuration and/or frequency of Custom-Pak use can/should be adjusted to reduce that differential, or an alternative means of surgical supply procurement and management should be used.
The sensitivity analyses reveal that the BIM is independently robust to: a) changes in the job title (and resulting salary) of the staff assigned to a particular task, b) the number of staff who complete each task, and c) substantial variation in total costs. These findings suggest that the model is generalizable to facilities and other countries with varied title-task assignment arrangements, size of their workforce devoted to managing surgical supplies and surgery preparation, and/or total annual costs for conducting cataract and retina procedures in a community hospital setting. Therefore, we expect appreciable indirect cost savings are possible across most hospitals performing cataract and retina procedures, which are substantial when extrapolated provincewide and countrywide.
Using comprehensive surgical packs for ophthalmological procedures can standardize medical supply sourcing which can positively affect patients, staff, and the hospital. Custom comprehensive packs support the intuitive nature of surgery by providing flexibility of supply use at the individual level, allowing surgeons to have access to the instruments that are ideally suited to them personally, improving procedural efficiency. Using standard procedural practices may reduce opportunity for error and variation in care, ultimately improving outcomes.21 Optimizing OR supply inventory can improve inventory stability and reduce the number of inventory touch points,2 as well as improve workflow and labor productivity.22 Because supply expenses are the majority of the perioperative expense budget, more efficient supply chain management can result in cost savings.23 Limiting the number of sources from which medical supplies are purchased can provide quantitative benefits such as reduced cost and waste, and qualitative benefits including reducing variation in clinical practice.24 Surgical packs that include single-use equipment-specific surgical supplies can potentially improve patient safety if the alternative is reusing single-use devices to address budget and supply shortage concerns, as has been demonstrated in a study of phaco handpiece tips used in cataract surgery.25 Although not assessed in our model, full utilization of comprehensive Custom-Pak could potentially improve the quality of ophthalmological surgeries by reducing contamination of supplies versus use of generic commodity packs requiring the handling of additional individual supplies with varying levels of sterility;5 potential reduction of waste and time spent on waste management could be additional benefits.
Increased use of comprehensive surgical packs can also reduce the number of patients on the waiting list for procedures if time savings enable the completion of more procedures – this addresses three of the six quality domains evaluated by the Ontario Ministry of Health based on the QBP policy objectives: efficiency, access, and patient-centeredness. In Ontario, where 125,873 cataract QBP clinical cases were performed in 2019/2020,11 if all of the time savings gained from full utilization of comprehensive Custom-Pak were efficiently used to perform additional procedures, this potentially translates to 9858 additional procedures which could help mitigate the backlog of procedures due to the COVID-19 pandemic.11,15 Reducing wait times is a key focus for the Ontario Ministry of Health and Long-Term Care for several priority areas including cataract surgery,26 as increased wait times may potentially result in more complicated and costly procedures.13 Wait time reduction could be particularly critical as the population ages and the demand for ophthalmological surgery increases.14 An analysis of future cataract surgery rates in Ontario estimated the need for cataract surgery could double between 2010 and 2036, requiring a growth in surgical volume of 128%.27 Based on the findings from The Cost of Vision Loss and Blindness in Canada 2021 report, the Canadian Council of the Blind and Fighting Blindness Canada recommends that Canada improves access to treatments, including eye surgeries, for treating eye diseases that can lead to blindness.13
There are limitations to this study. As the sampling method for the US survey was not random, there may potentially be self-selection bias and/or sample selection bias. Respondents (or their institutions) taking part in the US study may look different than those in Canada due to time restraints, institutional policies, or other factors. The US data used in this research was self-reported; although potentially less reliable than third-party observation, this approach allowed for the collection of data from numerous facilities. Winsorizing controlled for outliers at the top of the data distribution which also reduced variation in the data; thus, the analysis is more likely to underestimate than overestimate savings assessments. Time estimates per procedure and per year were indirectly calculated based on the US survey using a series of questions regarding available information such as the typical time to complete the broadest task, the share of time spent on each subtask, and the typical time/share of time; we used these inputs to calculate the time for each subtask. The Canadian data included in the BIM was primarily sourced from one facility in Ontario, thus the generalizability may be limited if there are variations in protocols at other facilities conducting cataract and retina surgery across Canadian provinces and territories. However, in 2012, Kensington Eye Center had the second largest volume of cataract surgeries in Ontario28 and as of 2019, approximately 34% of all cataract day surgeries and 40% of all ophthalmic services in Canada were conducted in that province.13,28 Departmental processes, number and/or type of personnel responsible for the tasks accounted for in the BIM, and tasks needed to procure, manage, and use surgical supplies for cataract and retina surgeries may vary across other facilities in Canada. Generalizability will also be limited if the amounts of each surgical supply typically used in each surgery differs in Canada or if the time recorded by US sources is appreciably different than in Canada regarding worker productivity, education/training requirements, quality of surgical technology, or culture related to speed/procedure volume. Additionally, this study did not examine safety, outcomes, or environmental impacts of surgical packs; these could be explored in future research.
Lastly, we made several assumptions regarding the measurement and management of comprehensive Custom-Pak itself. We assumed that timing estimates for comprehensive Custom-Pak are adequately represented by the average configuration and timing estimates across all Custom-Pak measures. This implies that including additional supplies within the Custom-Pak does not substantially increase the time spent handling the pack overall. We also assumed that increased Custom-Pak usage results in larger orders rather than additional orders placed.
Conclusions
The use of comprehensive custom packs for cataract and retina surgery can streamline the sourcing of surgical supplies and provide substantial time and cost benefits to hospital facilities in Canada. By improving efficiency both peri-operatively across the accounting and materials management departments and during surgery preparation in the OR, comprehensive surgical pack use can reduce hidden costs. These savings may allow surgical staff to devote more time to other aspects of the procedure and patient care and may increase the number of surgeries that can be performed, directly benefiting patients by reducing wait list times.
Abbreviations
BIM, budget impact model; CAD, Canadian Dollar; KEI, Kensington Eye Institute; OR, operating room; QBP, Quality Based Procedures; US, United States.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the proprietary and confidential nature of the data, but the models and methodology can be obtained from the corresponding author on reasonable request. Data is available on file at Alcon.
Ethics Approval and Informed Consent
Western Institutional Review Board reviewed the study and considered it exempt because it is an online survey with adequate protections in place to protect the privacy of subjects and to maintain the confidentiality of data. The study and data accumulation were in conformity with all country, federal, or state laws, informed consent was obtained from participants, and the study was in adherence with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge John Yip (president and chief executive officer) and Thuong Huynh (manager) of Kensington Eye Institute (KEI, part of Kensington Health) for sharing their expertise and information related to KEI for this study.
Author Contributions
JSD made substantial contribution the conception and study design. DP and JSD made substantial contribution to the acquisition of data. JSD was primarily responsible for the statistical analysis of the data. All authors were responsible for analysis and interpretation of the data. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Alcon Canada, Inc., which also funded the medical writing support provided by KJT Group, Inc.
Disclosure
Ms Punch is a consultant for Alcon and Kensington Eye Institute. Mr Gill, Ms Hsiao, and Dr Kara are employees of Alcon, the sponsor of this research. Ms Hahn is an employee of KJT Group, Inc. which was contracted by Alcon to conduct the study and provide medical writing support. At the time the study was conducted, and the manuscript was written, Mr Davis was an employee of KJT Group, Inc. The authors report no other conflicts of interest in this work.
References
1. Harmer BA. The hidden cost calculator: a new way to look at custom packs. Mater Manag Health Care. 1995;4(7):18–19.
2. Market Scope. Single-use ophthalmic surgical products market report: a global analysis for 2019 to 2025; 2020.
3. Dexter F, Abouleish A, Epstein R, Whitten C, Lubarsky D. Use of operating room information system data to predict the impact of reducing turnover times on staffing costs. Anesth Analg. 2003;97:1119–1126. doi:10.1213/01.ANE.0000082520.68800.79
4. Krupka D, Sathaye S, Sandberg W. Reducing non-operative time: methods and impact on operating room economics. Int J Healthc Technol Manag. 2008;9(4):1. doi:10.1504/IJHTM.2008.019672
5. Cardoen B, Beliën J, Vanhoucke M. On the design of custom packs: grouping of medical disposable items for surgeries. Int J Prod Res. 2015;53(24):7343–7359. doi:10.1080/00207543.2015.1061221
6. Gonzalez TA, Bluman EM, Palms D, Smith JT, Chiodo CP. Operating room time savings with the use of splint packs: a randomized controlled trial. Arch Bone Joint Surg. 2016;4(1):10–15.
7. Lafuma A, Smith AF. PES13 A cost minimisation analysis of custom pak®for cataract surgery. Value Health. 2004;7(6):749. doi:10.1016/S1098-3015(10)65990-6
8. Government of Canada. Canada’s Health Care System; 2021. Available from: https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-system/canada.html.
9. Canadian Institute for Health Information. National health expenditure trends; 2020. Available from: https://www.cihi.ca/sites/default/files/document/nhex-trends-2020-narrative-report-en.pdf.
10. Jacobs J, Daniel I, Baker G, Brown A, Wodchis W. Bundling care and payment: evidence from early adopters. Available from: https://www.oha.com/Documents/2434_OHA_Bundling_Care_Payment_Policy_Paper.pdf.
11. Ontario Provincial Vision Task Force and Ministry of Health. Quality-based procedures clinical handbook for cataract day surgery. Available from: https://www.health.gov.on.ca/en/pro/programs/ecfa/docs/qbp_cataract.pdf.
12. Government of Canada. Health Canada procurement plan (assets and acquired services) 2019–2020; 2021. Available from: https://www.canada.ca/en/health-canada/corporate/transparency/corporate-management-reporting/report-plans-priorities/2019–2020-procurement-plan.html.
13. Canadian Council of the Blind. The cost of vision loss and blindness in Canada: summary report recommendations. Available from: https://www.fightingblindness.ca/wp-content/uploads/2021/05/Deloitte-Final-Acc-of-VL-and-Blindness-in-Canada-May-2021.pdf.
14. Jin S, Chan SWS, Gupta N. Distribution gaps in cataract surgery care and impact on seniors across Ontario. Can J Ophthalmol. 2019;54(4):451–457. doi:10.1016/j.jcjo.2018.10.022
15. Felfeli T, Ximenes R, Naimark DM, et al. Predicting the ophthalmic surgical backlog as a result of the COVID-19 pandemic: a population-based study and microsimulation model to inform surgical recovery plans. medRxiv. 2021;2021:1. doi:10.1101/2021.03.25.21254375
16. Ayres BD, Gupta OP, Davis JS, et al. Economic impact analysis of custom pak® on cataract and vitreoretinal surgery in the United States. Clin Outcomes Res. 2022;14:715–730. doi:10.2147/ceor.s382188
17. Sadri H, Sinigallia S, Shah M, Vanderheyden J, Souche B. Time-driven activity-based costing for cataract surgery in Canada: the case of the Kensington eye institute. Healthcare Policy. 2021;16(4):97–108. doi:10.12927/hcpol.2021.26496
18. Kinney GJ, Lutjens LR. Cost accountability in the OR. A case for custom-designed, procedure-ready packs. AORN J. 1986;43(6):1306. doi:10.1016/s0001-2092(07)65160-6
19. Rusynko BS, Schall B. Custom open heart packs: evaluating their use in the OR. AORN J. 1984;40(3):379–384. doi:10.1016/s0001-2092(07)65375-7
20. Kensington Health. The Kensington eye institute year in review 2015–16. Available from: https://issuu.com/kensingtonhealth/docs/2015-kei-web.
21. Ontario Hospital Association. Optimizing your perioperative supply Chain: a guide to improvement projects. Available from: https://www.deslibris.ca/ID/230868.
22. Healthcare Financial Management Association. Achieving operating room efficiency through process integration. Healthc Financ Manag. 2003;57(3):112.
23. Park KW, Dickerson C. Can efficient supply management in the operating room save millions? Curr Opin Anaesthesiol. 2009;22(2):242–248. doi:10.1097/ACO.0b013e32832798ef
24. Mullins D, Persaud E, Ferko N, Knight B, Tripodi D, Delatore P. SKU Optimization Initiatives Can Create Cost Savings in an Era of Value-Based Care. Healthcare Financial Management Association; 2021. Available from: https://www.hfma.org/topics/hfm/2019/february/62987.html.
25. Cecchini P, D’Aloisio R, Antonuccio M, et al. Chemical and physical analysis of phaco handpiece tip surfaces before and after cataract surgery. J Cataract Refract Surg. 2017;43(8):1107–1114. doi:10.1016/j.jcrs.2017.05.027
26. Trypuc J, Hudson A, MacLeod H. Ontario’s wait time strategy: part 1. Healthc Q. 2006;9(2):44–51. doi:10.12927/hcq.2006.18101
27. Hatch WV, Campbell Ede L, Bell CM, El-Defrawy SR, Campbell RJ. Projecting the growth of cataract surgery during the next 25 years. Arch Ophthalmol. 2012;130(11):1479–1481. doi:10.1001/archophthalmol.2012.838
28. The Provincial Vision Strategy Task Force. A vision for Ontario: strategic recommendations for ophthalmology in Ontario; 2013.
29. Ontario Ministry of Health. Call for applications to license independent health facilities for the provision of cataract surgeries in Ontario. application guidelines; 2020.
30. Ontario Ministry of Health. Schedule of benefits. physician services under the health insurance act; 2020.
31. Statistics Canada. Table 14–10-0043-01. Average usual and actual hours worked in a reference week by type of work (full- and part-time), annual; 2021. https://doi.org/10.25318/1410004301-eng.
32. Statistics Canada. Table 14–10-0307-01Employee wages by occupation, annual, inactive; 2021. Available from: https://doi.org/10.25318/1410030701-eng.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.